
AbCellera Biologics

Thesis
AbCellera has four drugs in its pipeline across various stages of development; two in clinical trials and two in the R&D stage. The bull case hinges on the success of their flagship drug, ABCL635. I am betting this drug will be effective for reducing hot flashes in menopausal women. The results are expected in Q3 2026 after the completion of Phase 2 clinical trial. I expect the stock will re-rate quickly after the results. Up or down is the multi billion dollar question. I bought calls that expire on January 15, 2027 with a strike price of $7 to express my view on this binary outcome.
Drugs
ABCL635 - drug for hot flashes, Phase 1 completed, Phase 2 pending
ABCL575 - drug for atopic dermatitis, Phase 1 pending
ABCL688 - autoimmune drug targeted for Phase 1 in 2027 (details undisclosed)
ABCL386 - oncology drug targeted for Phase 1 in 2027 (details undisclosed)

ABCL635 is an antibody drug that targets NK3 receptors on KNDy neurons. Its function is to block these receptors to alleviate symptoms of VMS (hot flashes). Now, there are two other drugs on the market that target the same receptor: Fezolinetant (Veozah) by Astellas and elinzanetant (Lynkuet) by Bayer. After extensive research comparing the three, my conclusion is that ABCL635 wins on modality, safety, and technology. Efficacy is the one dimension I must speculate on until Phase 2 is complete. Ironically it's also the most important.
Modality
Fezolinetant and elinzanetant are small molecule oral pills taken daily while ABCL635 is a monoclonal antibody that’s administered as a monthly injection. AbCellera’s bet is that patients will trade popping pills on the daily for a monthly shot. This is made possible by the extended half life of the drug; 24 days vs 9-15 hours for the competitors1.
Safety
Fezolinetant carries risk of severe liver toxicity and the FDA put a warning label on the product2. Elinzanetant is clear on that front, but has somnolence (drowsiness), vertigo, diarrhea and more as known side effects3. ABCL635’s Phase 1 showed no observed liver toxicity or any serious adverse effects in 56 healthy volunteers4. AbCellera argues that an antibody, being too large to cross the blood-brain barrier, should avoid the CNS side effects (like somnolence and vertigo) that small molecules can trigger.
Technology
Small molecules vs antibodies. Time for a brief biology lesson. Small molecules have been around forever (100+ years), they are the pills found ubiquitously in medicine cabinets and local drug stores. Think tylenol, aspirin, adderall. Basically any type of pill most people have taken in their lives. Antibodies are the new kids on the block, and the fastest growing category in biopharma5. Let’s get into the weeds some more. Small molecules, like the name implies, are small (900 daltons). Small enough to slip past the blood brain barrier and get inside cells. On the other hand, antibodies are much bigger (150,000 daltons) and cannot cross the blood brain barrier or cell wall. This is advantageous because it makes them very selective. Antibodies bind to a single target and only that target, while small molecules tend to hit multiple targets at once, which is why they have more side effects, like the liver toxicity in fezolinetant and drowsiness/vertigo in elinzanetant. Simply put, carpet bombing vs a guided precision missile for taking out a target. If it was your body, which would you want? It is no wonder why antibodies are taking market share from small molecules in high value therapeutic areas.
Efficacy
Fezolinetant (45mg) reduced VMS by 2-3 hot flashes per day vs. placebo, meeting the FDA’s clinical threshold for a reduction of at least 2 VMS per day.6 Elinzanetant (120mg) reduced VMS by 1.8 hot flashes per day vs. placebo, and also got approved by the FDA7. Although ABCL635’s efficacy has yet to be determined, Phase 1 data is promising. It showed “greater absolute reduction and sustained suppression of testosterone with ABCL635 compared to fezolinetant Phase 1”. What does testosterone suppression have to do with efficacy? Well, it’s an early signal that ABCL635 is hitting its target, indicating the drug engages the target better than the leading competitor. The caveat is we still have to wait for Phase 2 results to get confirmation of efficacy.
Phase 1 Results & Phase 2 Expectations
Looking at industry wide data, Phase 2 success rate is ~30-35%8. These odds are significantly increased if certain signals are present in Phase 1. Strong positive predictors of Phase 2 are as follows.
Robust target engagement at tolerated doses
Wide therapeutic window
Clean safety profile
Predictable PK with low variability
Validated mechanism
Surrogate biomarker that correlates with clinical outcome
Does ABCL635 have these indicators? I will break it down one bullet point at a time. Phase 1 proved the drug has strong target engagement via sustained suppression of testosterone over a four week period. The therapeutic window is indeed wide since doses ranging from 30mg to 900mg were tested9. It has a clean safety profile as I mentioned before, no hepatoxicity or CNS effects. ABCL635 showed favorable linear pharmacokinetics (PK) across doses, with low variability and an estimated half-life of ~24 days10. Linear and low-variability means dose response in patients should be predictable. Mechanism was already validated by fezolinetant and elinzanetant. ABCL635 targets the same receptor (NK3) that has been proved to suppress VMS. No re-inventing the wheel here. Finally, testosterone suppression is a high signal biomarker that is predictive of target outcome. AbCellera’s drug scores well on all Phase 1 predictors, pushing the probability of a successful Phase 2 well above the median to ~60-75%11. This is assuming the central question in the next section resolves favorably.
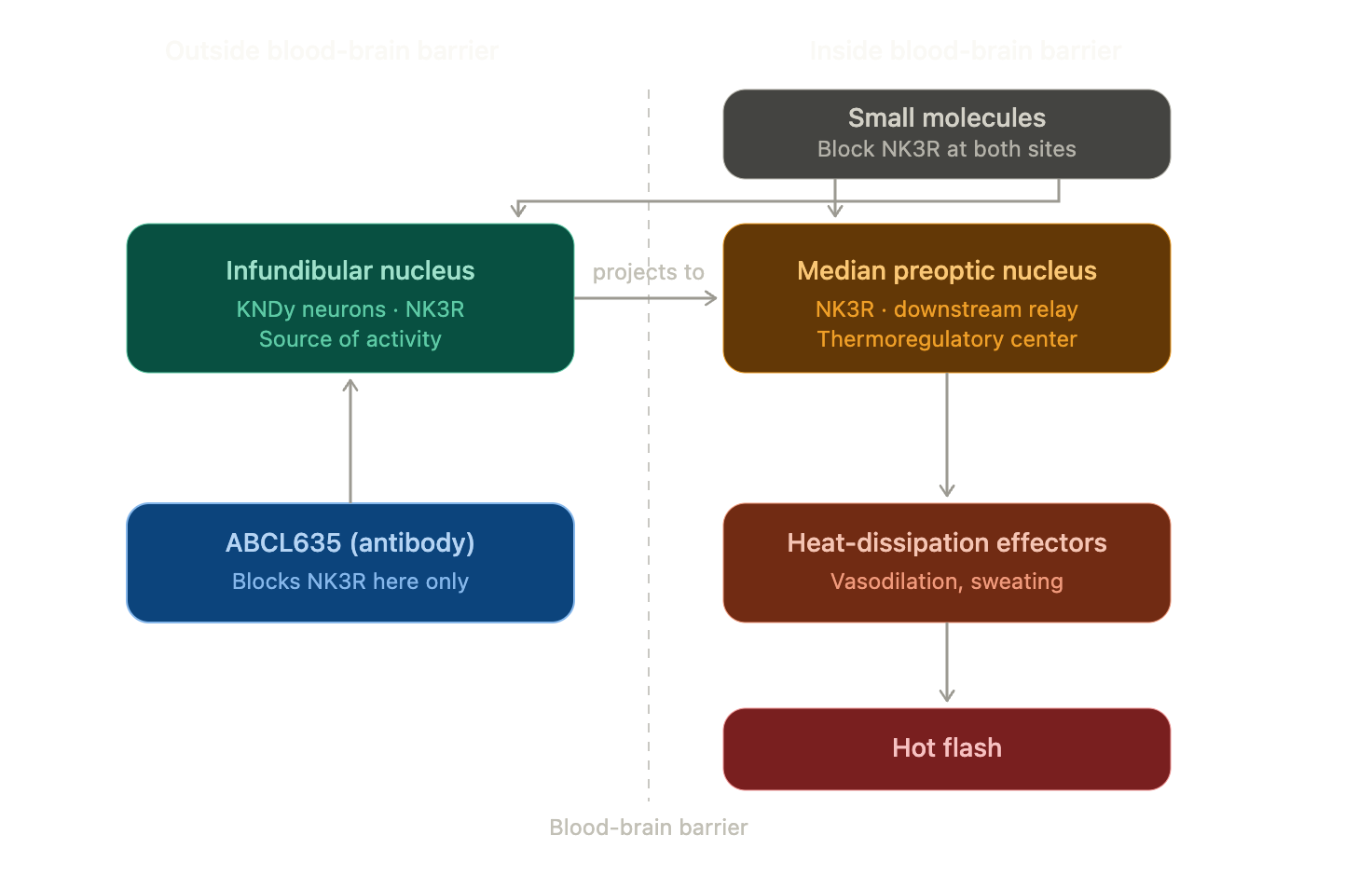
The Scientific Dilemma
Now there is one thing that could potentially de-rail the whole thing in terms of Phase 2 efficacy. It’s heavy on the science so I’ll go slowly. If you’ve been paying attention so far you should be aware that ABCL635 and the two competing drugs work by blocking NK3 receptors. The problem is that a lot of NK3 receptors, including a major one called the median preoptic nucleus (MnPO), are inside the blood brain barrier. ABCL635 cannot penetrate the blood brain barrier due to its large size. So if AbCellera’s drug can’t get in there and block these receptors, then how do they expect it to work? Well, some NK3 receptors are outside the blood brain barrier, like the hypothalamic infundibular nucleus, which is a very important one and the main binding target of ABCL635. So the competition’s small molecules are able to target both key receptors, but ABCL635’s antibody design can only target one. This is starting to look like a serious problem. So I ask myself:
Is blocking NK3R in the infundibular nucleus sufficient to meaningfully reduce hot flashes, or does it have to be blocked in the preoptic nucleus as well?
This is the single most important scientific question for this investment. The answer will be revealed in AbCellera’s Phase 2, but as a speculative investor I cannot wait that long. I need enough information to make an educated guess today. So, I had my LLM agent scour the internet for any pertinent scientific papers that would give me an edge. I found some very enlightening animal studies that point towards two models. There are two competing hypotheses that attempt to answer the question and each is backed by reputable studies.
Median Preoptic Nucleus (MnPO) Model
This is the approach taken by fezolinetant and elinzanetant. A study conducted by Astellas on rats found that “fezolinetant attenuates hot flash-like symptoms via inhibition of neuronal activity in the MnPO”12. Another study shows “that NK3R neurons in the MnPO are required for the hypothermic effects of senktide” solidifying MnPO’s importance in alleviating VMS13. If this model is correct, then AbCellera’s drug, which cannot reach the MnPO, would have limited efficacy. However, it does not establish that the MnPO must be blocked directly. It can be blocked indirectly by suppressing the infundibular nucleus, assuming it is upstream of the MnPO (model two). So this model does not conclusively determine that ABCL635’s approach will not work.
Infundibular (arcuate) Nucleus Model
AbCellera has chosen this model as the foundation for their drug and it hinges on the infundibular nucleus being the source of KNDy activity and upstream of the MnPO. The 2012 Mittelman-Smith rat study showed “KNDy neuron ablation consistently reduced tail-skin temperature, indicating that KNDy neurons facilitate cutaneous vasodilatation, an important heat dissipation effector”14. Translation, KNDy neurons in the infundibular nucleus play a huge role in regulating heat, which is positive for a drug that aims to reduce hot flashes. Furthermore, several animal studies place the MnPO downstream of arcuate KNDy neurons15. These suggest the source of activity causing hot flashes is in the infundibular nucleus and blocking it there should reduce VMS without directly targeting the MnPO, which sits downstream. If this model holds, Phase 2 should show ABCL635 reduces hot flashes.
Today, nobody can conclusively state which model is correct. No human study has tested blocking NK3R solely in the infundibular nucleus. ABCL635’s Phase 2 will be the first. I am, of course, leaning towards model two, so it is my educated guess that blocking NK3R in the infundibular nucleus is sufficient to meaningfully reduce hot flashes.
VMS Market
Most women experiencing hot flashes use estrogen pills/patches, not fezolinetant or elinzanetant, and they have significantly higher efficacy rates16. So why bother making these drugs and who is it for? Estrogen therapy comes with its own slew of side effects that make fezolinetant’s liver toxicity look tame. Breast cancer, blood clots, stroke and venous thromboembolism are a few of the rare, but very real side effects17. Many are fine taking estrogen but some are not. NK3 drugs are intended for women with a history of certain types of cancer, blood clots, stroke and as an alternative for estrogen. The TAM (total addressable market) for NK3 drugs is hard to quantify. Numbers vary ranging from $2B to $25B. I’d probably go with the lower end of it. Yes, it’s a niche market.
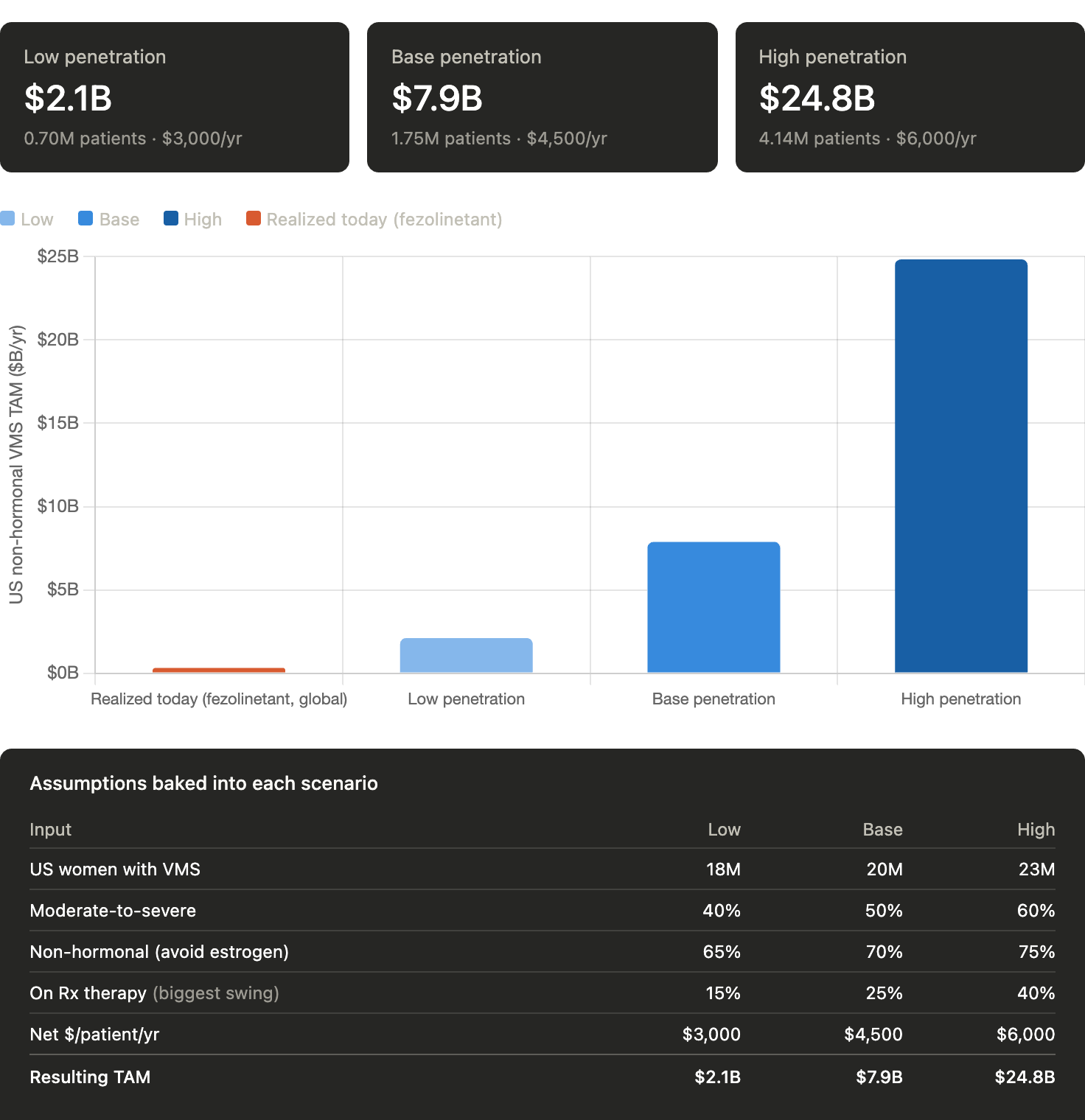
Fezolinetant is the current market leader, with sales growing from ¥7.3 billion ($50M) in FY2023 to ¥33.8 billion ($222M) in FY2024 and ¥46.6 billion ($309M) in FY202518. Elinzanetant has no commercial data yet and should expand the overall market as it becomes widely available. Fezolinetant's ramp shows real and accelerating commercial demand for NK3 drugs. If ABCL635 proves to be effective, its advantages in modality, safety, and technology give it a credible path to compete for share in a market fezolinetant has already shown is real.
Almost all successful silicon valley companies had some model of starting with small markets and expanding — Peter Thiel19
AbCellera’s strategy of starting with the niche VMS market and expanding to much bigger markets through its pipeline of drugs is taken right out of Thiel’s playbook. Not surprising since he was on the board for four years. I am an advocate of this strategy and it’s another reason why I’m long. ABCL635 is the company’s first stepping stone towards becoming a biotech juggernaut.
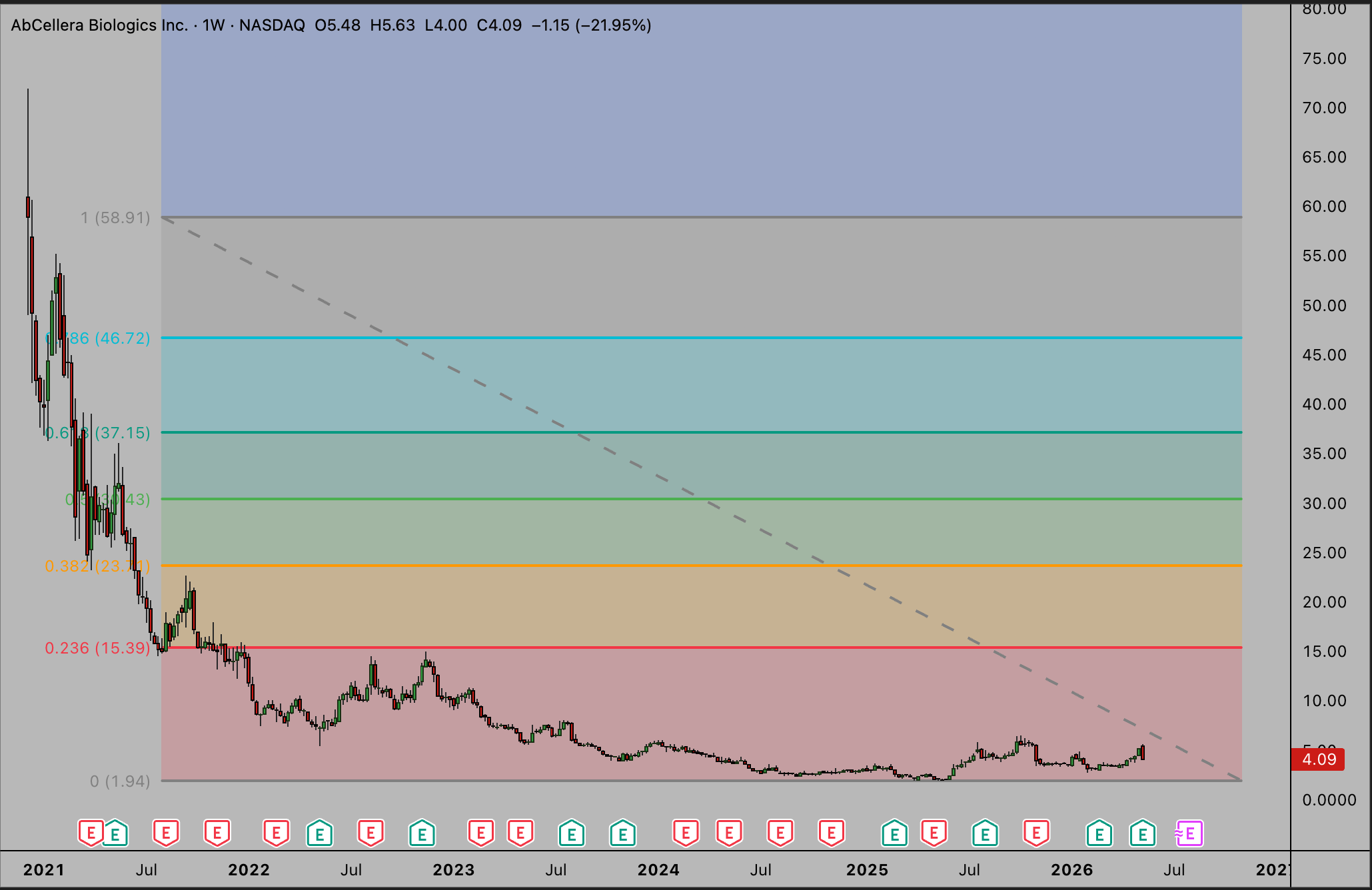
Technical Analysis & Exit Plan
I’m no TA wizard, but I know a multi-year accumulation chart with a catalyst for a breakout when I see one. The breakout has not happened yet and is speculative, but it would make for a very clean setup technically if Phase 2 succeeds. I can see the stock move quickly to the 0.236 Fibonacci level of ~$15 and possibly even higher to next level at ~$23 by end of 2026. I would likely sell a majority, if not all of my position in this range. If fundamentals look good further down the line, like ABCL575 has good news from its Phase 1 or the other drugs in the pipeline are progressing well, I may buy shares and become a diamond handed bag holder to ride this company into the next decade.
https://pmc.ncbi.nlm.nih.gov/articles/PMC11955179/
https://pubmed.ncbi.nlm.nih.gov/38869992/
https://www.ncbi.nlm.nih.gov/books/NBK608428/
https://www.ncbi.nlm.nih.gov/books/NBK620403/
https://www.businesswire.com/news/home/20260511135503/en/AbCellera-Reports-Q1-2026-Business-Results-Announces-Positive-Interim-Phase-1-Clinical-Data-for-ABCL635
https://pmc.ncbi.nlm.nih.gov/articles/PMC10535987/
https://pmc.ncbi.nlm.nih.gov/articles/PMC10348473/
https://www.endocrinologyadvisor.com/news/elinzanetant-safe-efficacious-in-treating-hot-flashes-through-1-year/
https://massivebio.com/phase-ii-iii-clinical-trial-bio/
https://s21.q4cdn.com/223776925/files/doc_financials/2026/q1/Updated_2026-Q1-FY-Business-Update-May-2026.pdf
Ibid
I made these numbers up
https://pubmed.ncbi.nlm.nih.gov/34048742/
https://pubmed.ncbi.nlm.nih.gov/25825817/
https://www.pnas.org/doi/10.1073/pnas.1211517109
https://pubmed.ncbi.nlm.nih.gov/29996088/ https://pmc.ncbi.nlm.nih.gov/articles/PMC2823949/
https://www.pnas.org/doi/10.1073/pnas.1211517109
https://pubmed.ncbi.nlm.nih.gov/15495039/
https://pubmed.ncbi.nlm.nih.gov/12117397/
¥145/¥152/¥151 exchange rates used for 2023/2024/2025
https://www.astellas.com/content/dam/astellas-com/global/en/confidential-documents/financial-results/4q2025_pre_en.pdf
https://www.astellas.com/content/dam/astellas-com/global/en/documents/financial-results/full-year-and-4q-fy2024-financial-results-en.pdf
https://www.astellas.com/content/dam/astellas-com/global/en/documents/financial-results/full-year-and-4q-fy2023-financial-results-en.pdf
youtube.com/watch?v=0C1H0_Uv1us
Great work